Fertility Tests for Women in India: A Complete Guide with What to Expect
What Fertility Tests Do Women Need in India?
-
-
- AMH (Anti-Müllerian Hormone) – measures ovarian reserve; can be done on any day of the cycle; simple blood draw
- FSH (Follicle-Stimulating Hormone) – assesses the brain’s signal to the ovaries; high FSH may suggest declining egg reserve
- LH (Luteinising Hormone) – the hormone that triggers ovulation; an elevated LH-to-FSH ratio can indicate PCOS
- Estradiol (E2) – baseline oestrogen level; contextualises FSH results; tested on Day 2–4 of the cycle
- TSH (Thyroid Stimulating Hormone) – checks thyroid function; silent hypothyroidism is very common in South Indian women and affects fertility
- Prolactin – elevated prolactin suppresses ovulation; best tested in the morning before exercise
- Transvaginal Ultrasound + Antral Follicle Count (AFC) – assesses uterine anatomy and counts active follicles; mild pressure, rarely painful
- HSG (Hysterosalpingography) – checks whether fallopian tubes are open; dye is injected through the cervix; mild cramping expected
- Follicular Monitoring Scans – series of ultrasounds across the cycle to confirm ovulation and track follicle growth
- Day 21 Progesterone – confirms whether ovulation has actually occurred; a simple blood draw
-
A complete basic fertility workup for a couple in India costs approximately ₹8,000–₹25,000 at a reputable clinic.
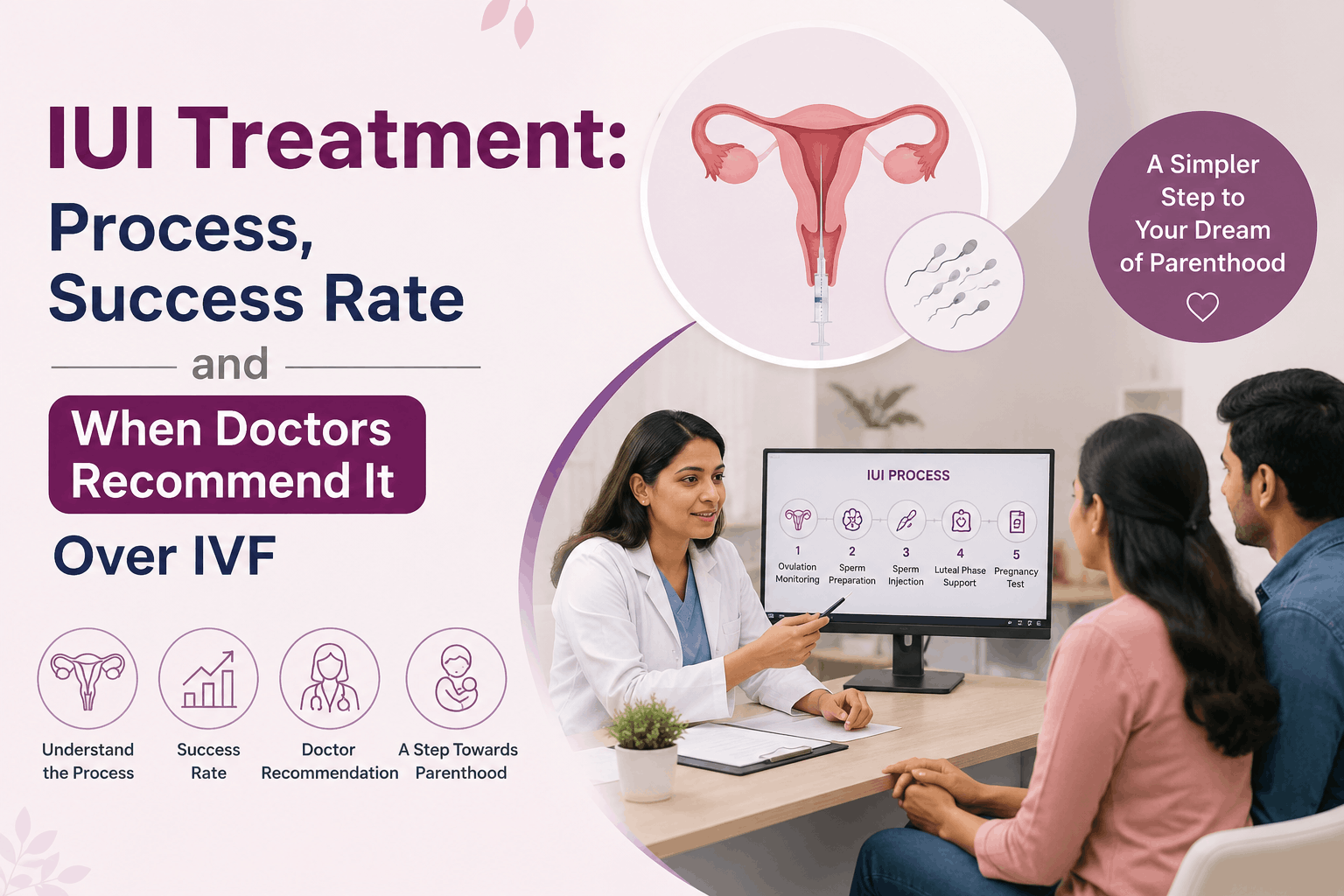
The moment a woman decides to check her fertility or is told she needs fertility tests, a single question takes over: what exactly will happen. But no one has explained what those tests actually are, what happens in the room, whether they will hurt, or how much they cost. The unknown creates anxiety, and anxiety keeps couples from taking the first step.
This guide is here to turn the unknown into the known. It covers every fertility test a woman might have, what it measures, when it is done, what to expect in the room, and approximate costs in India. Most of these tests are simple blood draws or ultrasound scans. Very few involve any discomfort. Understanding them in advance removes the fear and lets you walk into that first appointment confident and informed.
When Should You Get Fertility Tests?
Fertility testing is not one-size-fits-all. The right time depends on your age, how long you have been trying, and whether you have risk factors. Here is the practical guide:
|
Your Situation |
What to Do |
Why It Matters |
| Under 35, trying naturally | After 12 months without conceiving | 85% of couples without fertility issues conceive within 12 months; testing earlier may not be clinically indicated unless risk factors exist |
| Age 35 to 37 | After 6 months of trying | Egg quality and quantity decline with age; earlier investigation gives more options and time; every 6 months matters after 35 |
| Age 38 or older | Consider testing before trying, or after 3 months | Age is the single most important fertility factor; earlier access to results allows faster, better-informed decisions |
| Known risk factor (PCOS, endometriosis, irregular cycles, prior pelvic surgery, prior ectopic, recurrent miscarriage) | Before trying or at first decision to conceive | Risk factors predict a longer path to conception; early assessment avoids wasted time and allows targeted management |
| Planning to delay pregnancy (age 30 to 36) | Proactively at any point for baseline AMH and antral follicle count | AMH and AFC give a meaningful fertility timeline estimate; allows informed decision about egg freezing or earlier conception |
| Considering egg freezing | At consultation for egg freezing; ideally before age 35 | AMH and AFC determine stimulation protocol and expected egg yield; understanding baseline reserve is essential |
| Partner has abnormal semen analysis | Immediately; both partners assessed concurrently | Male and female factors frequently coexist; treating one without investigating the other leads to incomplete management |
Important note: Many women wait longer than clinically advisable before seeking assessment, often due to social reluctance or a belief that investigation implies something is wrong. This is a misconception. A fertility assessment gives information, not diagnoses. Understanding your fertility is empowering, whether or not you are currently trying to conceive.
Tier 1: The Basic Fertility Workup (First Consultation Tests)
These are the tests most women have at a first visit to a fertility specialist. They take a few hours total and give a complete picture of ovarian reserve, hormone balance, and uterine health.
|
Test |
What It Measures | When to Do It | What to Expect |
Cost (India, 2025) |
| AMH (Anti-Müllerian Hormone) | Ovarian reserve; how many follicles are active | Any day of cycle; NOT affected by cycle phase. Note: oral contraceptive pills suppress AMH artificially; inform your doctor if on the pill | Simple arm blood draw. No fasting. 5 to 10 minutes. Results in 24 to 48 hours. Normal range: 1.1 to 3.5 ng/mL | ₹1,200–3,000 |
| FSH (Follicle-Stimulating Hormone) | Brain signal to ovaries; high FSH suggests declining reserve | Day 2, 3, or 4 of menstrual cycle (first 4 days of period). Timing is critical. | Arm blood draw. No fasting. Often ordered with LH and Estradiol in one draw. Results within a day. | ₹300–800 (usually part of panel) |
| LH (Luteinising Hormone) | Ovulation trigger hormone; elevated LH-to-FSH ratio can indicate PCOS | Day 2 to 4 of cycle (same draw as FSH) | Arm blood draw. Part of combined panel with FSH and Estradiol. | ₹300–800 (usually part of panel) |
| Estradiol (E2) | Baseline oestrogen; contextualises FSH; high Estradiol can falsely lower FSH | Day 2 to 4 of cycle (same draw as FSH and LH) | Arm blood draw. Part of combined hormonal panel. | ₹300–700 (usually part of panel) |
| TSH (Thyroid Stimulating Hormone) | Thyroid function; hypothyroidism very common in South Indian women, often silent | Any day. Not cycle-dependent. Often tested in same draw as AMH. | Arm blood draw. Very common test; no special preparation. Target TSH for fertility: <2.5 mIU/L. Results next day. | ₹150–400 |
| Prolactin | Prolactin hormone; high levels suppress ovulation | Any day; ideally morning and without vigorous exercise or breast stimulation before test (both can temporarily raise prolactin) | Arm blood draw. Inform doctor of all medications before testing. | ₹200–500 |
| Transvaginal ultrasound (TVUS) + Antral Follicle Count (AFC) | Uterine anatomy; ovarian morphology; number of small follicles; detects fibroids, polyps, cysts, endometriomas | Day 2 to 5 of cycle for most accurate AFC; can be done at other times for uterine assessment | Ultrasound probe inserted vaginally; thin and well-lubricated; mild pressure sensation, rarely painful; 10 to 15 minutes; results shown and explained immediately; no sedation. | ₹1,500–3,500 |
Critical note about AMH and oral contraceptive pills: If you are currently taking the pill, your AMH result may appear lower than your true reserve. Always tell your doctor if you are on oral contraceptives before having this test. For the most accurate AMH, some doctors recommend stopping the pill for at least one cycle before testing, though this is not always necessary.
Tier 2: Tests Ordered When Specific Concerns Are Identified
These tests are not done at every first appointment. They are ordered when the initial workup suggests a specific issue or when your clinical history warrants it.
|
Test |
What It Measures | When to Do It | What to Expect |
Cost (India, 2025) |
| HSG (Hysterosalpingography) | Fallopian tube patency (whether tubes are open); uterine cavity shape | Days 7 to 10 of cycle (before ovulation; after period ends). Antibiotics may be prescribed before. | You lie on an X-ray table. A speculum is inserted (similar to a smear test). A thin catheter is placed through the cervix. Dye is injected; you may feel cramping similar to your menstruation. This lasts 10 to 20 minutes and passes within minutes. Pre-medicate with ibuprofen (400–600 mg) 1 hour before. Total time: 20 to 30 minutes. | ₹3,000–15,000 |
| SSG / HyCoSy (Sonosalpingography) | Tube patency using saline and ultrasound; no radiation | Days 7 to 10 of cycle. Alternative to HSG when radiation is avoided. | Saline injected via thin catheter; transvaginal ultrasound used to track flow; similar mild cramping to HSG; 15 to 20 minutes. | ₹2,000–6,000 |
| Follicular monitoring scan | Whether ovulation occurs; follicle growth pattern; endometrial thickness; confirms ovulation post-LH surge | Series of scans across the cycle: day 9 to 10, day 12 to 13, and again post-ovulation (day 17 to 21) in a typical 28-day cycle | Same as regular transvaginal ultrasound; 10 to 15 minutes per scan; 2 to 3 scans per cycle; results explained immediately. | ₹800–2,000 per scan |
| Progesterone (Day 21 / mid-luteal) | Confirms whether ovulation has occurred; levels ≥10 nmol/L (or ≥3.2 ng/mL) suggest ovulation | Day 21 of a 28-day cycle; adjust timing if cycle is longer (test 7 days before expected next period) | Simple arm blood draw; no preparation needed. | ₹200–500 |
| Hysteroscopy (diagnostic) | Direct view of uterine cavity; identifies polyps, fibroids inside cavity, septum, Asherman’s adhesions definitively | Done when ultrasound suggests an abnormality, or when unexplained implantation failure or miscarriage warrants investigation | Thin camera (hysteroscope) passed through cervix; mild cramping or pressure sensation; outpatient; local anaesthetic or mild sedation may be offered; 15 to 30 minutes; can be diagnostic and therapeutic in the same procedure. | ₹15,000–40,000 (outpatient diagnostic) |
Tier 3: Specialised Tests for Specific Diagnoses
These tests are not routine. They are ordered in specific clinical situations when Tier 1 and Tier 2 testing has pointed to a particular concern.
- Laparoscopy: Minimally invasive surgical procedure; gold standard for endometriosis and Fallopian tubal assessment; done under general anaesthesia; recommended when symptoms suggest endometriosis or when Tier 2 tests are inconclusive.
- Genetic karyotyping: Blood test for chromosomal analysis of both partners; recommended for recurrent miscarriage.
- Antiphospholipid antibody panel: For recurrent miscarriage investigation.
- Sperm DNA fragmentation: Male partner test; increasingly included when unexplained recurrent loss is present.
- Endometrial biopsy / ERA (Endometrial Receptivity Array): For repeated IVF implantation failure; identifies the personalised implantation window.
These are specialized tests ordered in specific clinical situations, not part of a standard first assessment.
What Your Male Partner Should Expect
Most first fertility consultations include the male partner. The primary test is semen analysis, which measures sperm count, motility (movement), and morphology (shape). The sample is collected through masturbation into a sterile container at the clinic or at home (must be delivered within 30 to 60 minutes). A 2 to 3 day abstinence period before the sample gives the most accurate results. Results are available within a few hours.
Male factor contributes to approximately 40 to 50% of infertility cases, so semen analysis is not optional. If the initial semen analysis is abnormal, additional male tests may be ordered: a hormone panel (FSH, LH, testosterone), a scrotal ultrasound, or a sperm DNA fragmentation test.
This is not about blame. Both partners are assessed together, and results are discussed as a couple with the treating doctor. Many cases of male infertility have effective treatments, particularly when diagnosed and addressed early.
Cost of Fertility Tests in India: 2026 Ranges
Basic hormone panel (AMH, FSH, LH, Estradiol, TSH, Prolactin): ₹2,000 to ₹8,000 depending on city and lab. Transvaginal ultrasound with antral follicle count: ₹1,500 to ₹3,500. HSG: ₹3,000 to ₹15,000. Follicular monitoring per scan: ₹800 to ₹2,000. Hysteroscopy (diagnostic outpatient): ₹15,000 to ₹40,000. Semen analysis: ₹500 to ₹1,500.
Total basic workup for a couple: approximately ₹8,000 to ₹25,000 at a reputable clinic. Many clinics in India offer bundled fertility assessment packages at slightly reduced cost. Always ask for an itemised breakdown of tests before proceeding, and ask what each test will tell you. You deserve to understand what you are paying for.
Quick Reference: Cycle Day Timing for Tests
|
When to Do Each Test |
Test Names |
| Any day of cycle (not timing-dependent) | AMH, TSH, Prolactin, Transvaginal ultrasound (for anatomy assessment) |
| Day 2, 3, or 4 of cycle | FSH, LH, Estradiol (must be early follicular phase for accuracy) |
| Day 5 to 7 of cycle | Transvaginal ultrasound for most accurate antral follicle count (AFC) |
| Day 7 to 10 of cycle | HSG (Hysterosalpingography) — must be before ovulation |
| Day 21 of cycle (or 7 days before expected next period if cycle is longer) | Progesterone (luteal phase — to confirm ovulation) |
What Happens After the Tests?
Results are reviewed together with your treating doctor, usually at a follow-up consultation. The doctor will explain what each result means in the context of your age, menstrual history, and symptoms, not in isolation. A single abnormal result is not a diagnosis. Most couples receive one of three outcomes: everything looks normal and you are advised to continue trying with monitoring; a specific finding is explained clearly with a targeted treatment plan; or further tests are needed for a specific concern.
Frame this as a conversation, not a verdict. At Sudha Fertility Centre, results are discussed with the doctor present, not sent as lab reports with no explanation. You will understand what the numbers mean and what the next step is before you leave.
Your First Appointment: What to Bring
Bring any previous medical records, a record of your menstrual cycle history (cycle length, regularity, any irregularities), a list of all medications and supplements you are taking (including the oral contraceptive pill if applicable), and any test results you may have had done previously. Write down any questions you want to ask before you arrive; it is easy to forget in the moment. If you are bringing your partner, make sure both of you are clear on what to expect.
The Path Forward
Fertility testing marks the beginning of understanding your fertility, not the end of your journey. Whether you are actively trying to conceive, planning ahead, or simply want to understand your fertility health, a first consultation at Sudha Fertility Centre is a conversation, not a commitment to treatment. Our specialists will review your history, recommend only the tests that are relevant for you, and explain every result clearly.
At Sudha Fertility Centre, Dr. S. Dhanabagyam and Dr. S. Pradeepa support you through every stage of this journey. A free first consultation is your chance to ask questions, understand your options, and make decisions that feel right for you and your family. Sudha has dedicated teams across Bangalore, Hyderabad, Chennai, and Coimbatore. If subsequent cycles are not successful or questions arise, the team will review what happened, discuss what can be adjusted, and outline the next steps before any further decisions are made.
Disclaimer: This article is for general informational purposes only and does not constitute medical advice. Fertility testing and management should always be done in consultation with a qualified fertility specialist based on individual clinical assessment.
Frequently Asked Questions
What is the first fertility test a woman should get in India?
At what age should a woman start fertility testing in India?
Does the AMH test require fasting or specific cycle timing?
Is the HSG test painful?
What does a normal AMH level mean for fertility?
How much do fertility tests cost in India?
Can fertility tests detect PCOS in women?
Do fertility tests hurt?
Can a woman with irregular periods still get fertility tests done?
Should the male partner also get tested at the same time as the woman?

Dr. S. Pradeepa is a fertility specialist at Sudha Fertility Centre, Erode, with expertise in IVF, IUI, ICSI, PCOS, and endometriosis. She holds MBBS, DGO, DNB (OG), and a Fellowship in Reproductive Medicine. Known for her patient-centric approach, she provides personalized, evidence-based care and reviews medical content to guide informed fertility decisions.