Adenomyosis vs Endometriosis: A Guide for Women Trying to Conceive
Being diagnosed with adenomyosis or endometriosis while trying to conceive can feel overwhelming. Both conditions affect the uterus and both connect directly to fertility challenges, but they differ in important ways. Many women are unsure which condition they have, how serious it is, or what it means for their chances of getting pregnant.
Understanding Adenomyosis vs Endometriosis clearly helps women ask the right questions, get the right tests, and make informed decisions about treatment and fertility. This guide covers the key differences, symptoms, diagnosis, and what both conditions mean for conception.
Understanding Adenomyosis and Endometriosis
What Is Adenomyosis?
Adenomyosis occurs when the tissue that normally lines the inside of the uterus grows into the muscular wall of the uterus itself. This causes the uterine muscle to thicken, which is why a thick uterus is one of the hallmark findings on ultrasound. The condition tends to cause painful and heavy periods and an enlarged uterus.
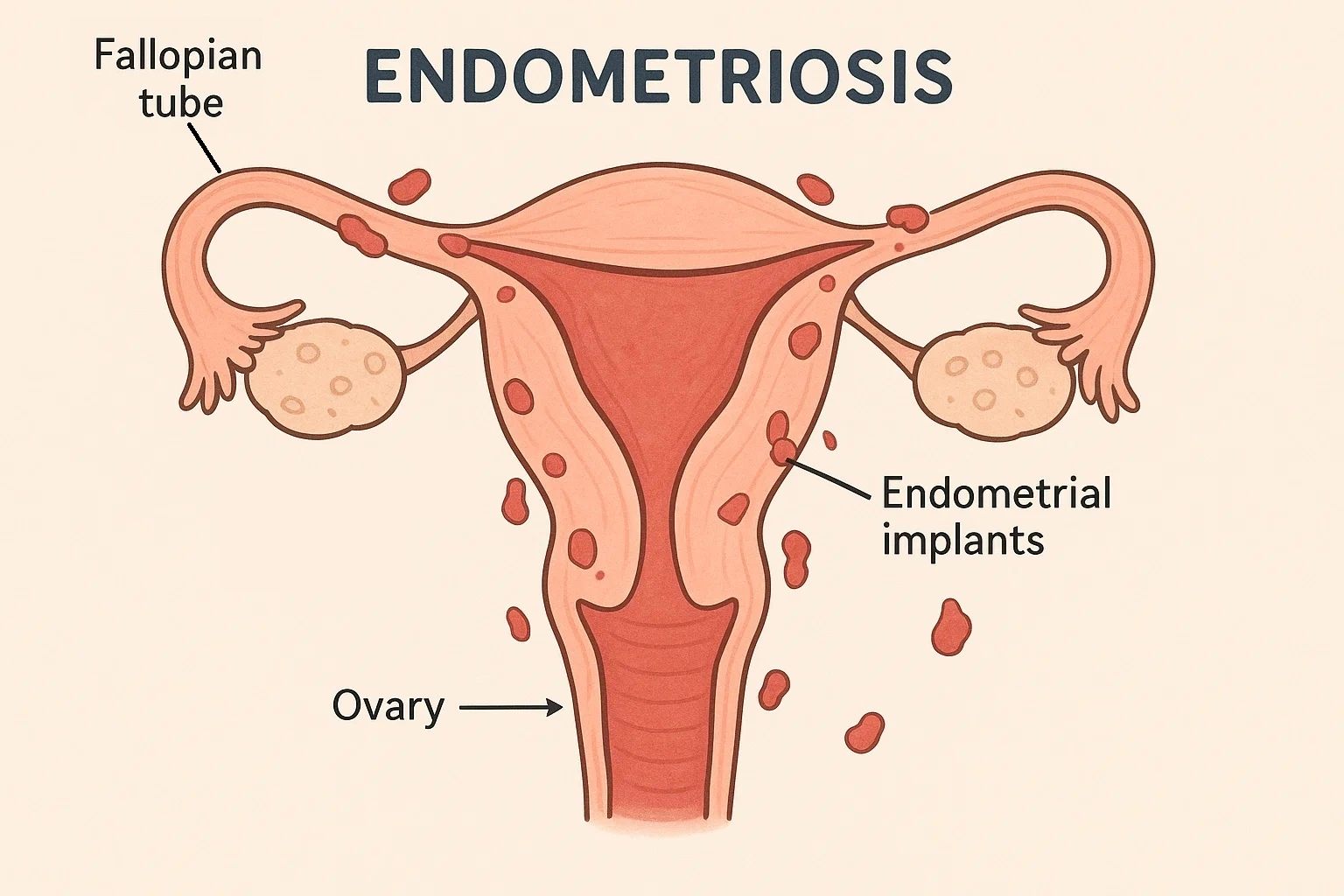
What Is Endometriosis?
Endometriosis occurs when tissue similar to the uterine lining grows outside the uterus, most commonly on the ovaries, fallopian tubes, and pelvic lining. This tissue responds to hormonal changes each month, causing inflammation, scarring, and uterine scar tissue and adhesions that can affect nearby organs and fertility.
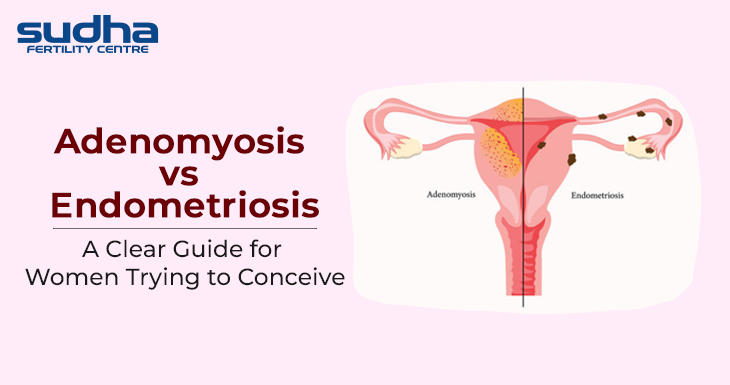
The Key Difference Between Adenomyosis and Endometriosis
The core difference between adenomyosis and endometriosis is location. In adenomyosis, abnormal tissue grows within the uterine wall. In endometriosis, it grows outside the uterus. Both cause pain and heavy periods, but endometriosis more directly affects the fallopian tubes and ovaries, while adenomyosis primarily disrupts uterine function and implantation.
Adenomyosis vs Endometriosis: Can You Have Both?
Yes. Research shows that a significant number of women with endometriosis also have adenomyosis. Having both conditions together tends to cause more severe symptoms and a greater impact on fertility. A thorough evaluation covering both is important rather than treating one while missing the other.
Adenomyosis vs Endometriosis vs Fibroids
Fibroids are non-cancerous growths of muscle and fibrous tissue that develop inside or around the uterus. Unlike adenomyosis and endometriosis, fibroids do not involve endometrial tissue growing in the wrong place. However, all three conditions can coexist, cause heavy painful periods, and affect fertility. The treatment approach differs for each, which is why accurate diagnosis matters.
Symptoms of Endometriosis and Adenomyosis
Both conditions share several overlapping symptoms, which is one reason they are often confused or diagnosed late. Common symptoms include:
- Heavy or prolonged periods: Both conditions cause heavy menstrual bleeding. In adenomyosis, a thick uterus leads to heavier and longer periods. In endometriosis, inflammation and scarring contribute to abnormal bleeding.
- Painful periods: Managing pain during periods is a major concern with either condition. The pain ranges from moderate cramping to severe pelvic pain that disrupts daily life.
- Chronic pelvic pain: Pelvic pain both during and after periods is a key symptom of endometriosis. Adenomyosis typically causes pain concentrated around menstruation.
- Pain during intercourse: Deep pain during intercourse is more commonly associated with endometriosis, particularly when tissue affects the uterosacral ligaments or ovaries.
- Bloating and bowel symptoms: Endometriosis affecting the bowel can cause bloating, constipation, or diarrhoea around periods. Adenomyosis causes more generalised abdominal discomfort.
- Uterine enlargement: A thick uterus and uterine enlargement are physical signs more specific to adenomyosis, typically detected on ultrasound or pelvic examination.
Stages and Severity
Doctors classify endometriosis into four stages based on the location, extent, and depth of tissue involvement. Stage 1 is minimal, Stage 2 is mild, Stage 3 is moderate, and Stage 4 is severe, often involving the ovaries, fallopian tubes, and surrounding structures. Higher stages are more likely to affect fertility directly.
Adenomyosis does not follow a universally agreed staging system, but doctors assess its severity based on how deeply the endometrial tissue has grown into the uterine muscle and how much of the uterine wall is involved. More extensive adenomyosis generally produces heavier symptoms and a greater impact on implantation and pregnancy outcomes.
How to Diagnose Adenomyosis and Endometriosis
Accurate diagnosis is essential because the treatment approach differs between the two conditions. Doctors use the following methods:
- Transvaginal ultrasound: The first investigation for both conditions. It detects a thick uterus, uterine enlargement, ovarian endometriomas (chocolate cysts), and signs of adenomyosis within the uterine wall.
- MRI: MRI provides a detailed view of adenomyosis within the uterine muscle and maps endometriosis deposits in complex or unclear cases.
- Laparoscopy: The gold standard for diagnosing endometriosis. A camera inserted into the abdomen lets the surgeon directly view and biopsy endometriosis lesions. Laparoscopy also allows treatment in the same procedure.
- Hysteroscopy: Used to examine the inside of the uterus and assess the impact of adenomyosis or uterine scar tissue on the uterine cavity.
Impact on Fertility
Can Endometriosis Cause Infertility?
Yes. Endometriosis causes infertility through multiple mechanisms. It damages the fallopian tubes through scarring and adhesions, reduces egg quality, creates an inflammatory pelvic environment hostile to fertilisation, and lowers ovarian reserve when it affects the ovaries. Studies estimate that 30 to 50 percent of women with endometriosis face fertility challenges.
How Adenomyosis and Endometriosis Affect IVF Success?
Both conditions reduce IVF success rates if left unaddressed. Adenomyosis reduces uterine receptivity and raises the risk of implantation failure and miscarriage. Endometriosis affects IVF through poor egg quality, reduced ovarian response, and tubal damage. With the right pre-treatment and surgical management where needed, IVF outcomes can improve significantly.
Chances of Conceiving Naturally
Natural conception is possible with both conditions, particularly in milder cases. Women with minimal to mild endometriosis and localised adenomyosis can conceive naturally. The chances decrease with the condition’s progression and age. Early evaluation and advanced treatment improve natural conception rates significantly.
Management and Treatment Options
Learning how to manage adenomyosis and endometriosis involves medical, surgical, and lifestyle approaches. Treatment depends on symptom severity, the extent of the condition, and whether the patient is trying to conceive.
- Hormonal therapy: GnRH analogues, progesterone therapy, and hormonal contraceptives suppress endometrial tissue growth and reduce pain. These are not used while actively trying to conceive but prepare the body before fertility treatment cycles.
- Surgery: Laparoscopy removes endometriosis lesions and adhesions. For adenomyosis, surgical options range from localised tissue removal to, in severe cases, hysterectomy for women who have completed their family.
- IVF: For women with significant tubal damage, poor ovarian reserve, or repeated implantation failure, IVF offers the most effective path to pregnancy. Both adenomyosis and endometriosis are factored into IVF protocol planning.
- Lifestyle and diet: An anti-inflammatory diet rich in omega-3 fatty acids, leafy greens, and low-glycaemic foods helps manage symptoms. Reducing alcohol, caffeine, and processed foods alongside regular moderate exercise supports both conditions.
- Natural approaches for endometriosis: For women trying to conceive with endometriosis naturally, maintaining a healthy weight, tracking ovulation, and reducing inflammatory triggers through diet are practical first steps alongside medical management.
When to see a specialist: If periods are consistently heavy or painful, pelvic pain is interfering with daily life, conception has not occurred after 6 to 12 months of trying, or either condition has already been diagnosed, a fertility evaluation is the right next step. Early intervention leads to better outcomes for both symptom management and conception.
Conclusion
Adenomyosis vs endometriosis is not just a medical comparison. For women trying to conceive, understanding the difference shapes every decision from diagnosis to treatment. Adenomyosis grows within the uterine wall and affects implantation. Endometriosis grows outside the uterus and can damage tubes, ovaries, and egg quality. Both are manageable with the right medical support.
Neither condition means pregnancy is impossible. With accurate diagnosis, targeted treatment, and specialist guidance, many women with adenomyosis or endometriosis go on to have successful pregnancies.
At Sudha Fertility Centre, Dr. S. Dhanabagyam and Dr. S. Pradeepa begin with a thorough diagnostic evaluation to find the exact cause and recommend the most suitable treatment path. If adenomyosis or endometriosis is affecting fertility, a structured evaluation is the clearest way forward.

Dr. S. Pradeepa is a fertility specialist at Sudha Fertility Centre, Erode, with expertise in IVF, IUI, ICSI, PCOS, and endometriosis. She holds MBBS, DGO, DNB (OG), and a Fellowship in Reproductive Medicine. Known for her patient-centric approach, she provides personalized, evidence-based care and reviews medical content to guide informed fertility decisions.